

Squamous cell carcinoma is the second most common skin cancer after basal cell carcinoma, It arises from the squamous cells that comprise most of the upper layer of the outer layer of the skin, the epidermis. Squamous cell cancers may occur on all areas of the body including the mucous membranes but are most common in areas exposed to the sun. Although squamous cell carcinomas are common on the skin, there are other squamous cells in other parts of the body including the lungs as well as all of the openings in the skin. Squamous cell carcinomas usually do not spread to other parts of the body as long as they are treated in a reasonable time.
What Causes It
Chronic exposure to sunlight causes most cases of squamous cell carcinoma. That is why tumors appear most frequently on sun-exposed parts of the body: the face, neck, bald scalp, hands, shoulders, arms, and back. The rim of the ear and the lower lip are especially vulnerable to the development of these cancers.
Squamous cell carcinomas may also occur where the skin has suffered certain kinds of injury: burns, scars, long-standing sores, sites previously exposed to X-rays, or certain chemicals (such as arsenic and petroleum by-products). In addition, chronic skin inflammation or medical conditions that suppress the immune system over an extended period of time may encourage the development of squamous cell carcinoma. Squamous cell carcinomas are the most common type of skin cancer in immunosuppressed patients such as transplant survivors.
Warning Signs of Squamous Cell Carcinoma
| -A wart-like growth that crusts and occasionally bleeds. | ||
| -A persistent, scaly red patch with irregular borders that sometimes crusts or bleeds. | ||
| -An open sore that bleeds and crusts and persists for weeks. | ||
| -An elevated growth with a central depression that occasionally bleeds. -PAIN – most squamous cell carcinomas are tender, often described as feeling like a burr or glass in the skin. This is unique to this kind of skin cancer. |
Squamous Cell Carcinoma – Treatment Options
If skin cancer is suspected, a biopsy must be taken and examined microscopically. When evaluating the biopsy, the pathologist tells us if we have “Clear margins” or not. If there is squamous cell carcinoma still present at the edges of the biopsy, then the “Margins are Involved” and further treatment is needed to make sure the squamous cell carcinoma is fully removed. There are many treatment options from which to choose. The choice of treatment is based on the type, size, location, and depth of penetration of the tumor, as well as the patient’s age and general state of health. Treatment can almost always be performed on an outpatient basis. A local anesthetic is used during most procedures. Pain or discomfort is usually minimal with most techniques, and there is rarely much pain afterward.
Topical Medications Two topical medications, Imiquimod (Aldara, Zyclara) and 5-FU (Efudex, Tolak, Carac), are approved for the treatment of superficial squamous cell carcinoma (also known as Bowen’s disease). These creams work to help trigger your immune system to fight off the tumor. These medications can be expensive and require use multiple times a week for about one month. The lesions can be ulcerated open sores and tender during the treatment process. This method can have excellent cosmetic outcomes but requires patient compliance with both applications of the medicine and the side effects of open healing lesions. This method is best used on large superficial lesions and lesions where cosmesis is a primary issue; however, this is only effective for some very superficial lesions. Dr. Rosenberger can prescribe these medications.
Curettage and Electrodesiccation The growth is scraped off with a curette and the tumor site desiccated with electrocautery. This method works because the tumor cells are not well adhered to the surrounding skin. This is not the most exact method of removal, because the margins of the removed tissue are not examined to determine that the entire tumor has been removed. However, this is an effective method for lesions on the trunk and limbs. This method is less often used on the central face because it does not leave the most cosmetically elegant scar. This method results in a pink or white circular scar somewhat larger than the original lesion. Dr. Rosenberger performs this technique in her office under local anesthesia.
Excisional Surgery Along with the above procedure, this is one of the most common treatments for BCCs and SCCs. Using a scalpel, the physician removes the entire growth along with a surrounding border of apparently normal skin as a safety margin. The incision is closed, and the growth is sent to the laboratory to verify that all cancerous cells have been removed and that the margins are clear. This method is used for lesions on the body as well as for lesions on the face. This method most often results in a sutured wound with a straight-line scar. The patient will need to return for suture removal. Dr. Rosenberger performs this technique in her office under local anesthesia.
Mohs Micrographic Surgery The physician removes the visible tumor and then removes very thin layers of the remaining surrounding skin one layer at a time. Each layer is checked under a microscope, and the procedure is repeated until the last layer viewed is cancer-free. It is often used for tumors that have recurred or are in hard-to-treat places such as the head, neck, hands, and feet. It is also used for lesions in high-risk locations such as the ear or the lip. This procedure requires additional training and equipment and is not performed by most general dermatologists. Dr. Rosenberger does not perform this procedure. However, she can refer you to a doctor who does perform this procedure. This technique has the highest cure rate and can save the greatest amount of healthy tissue. Therefore, this method has the best chance of minimizing scarring as well.
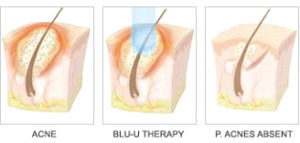
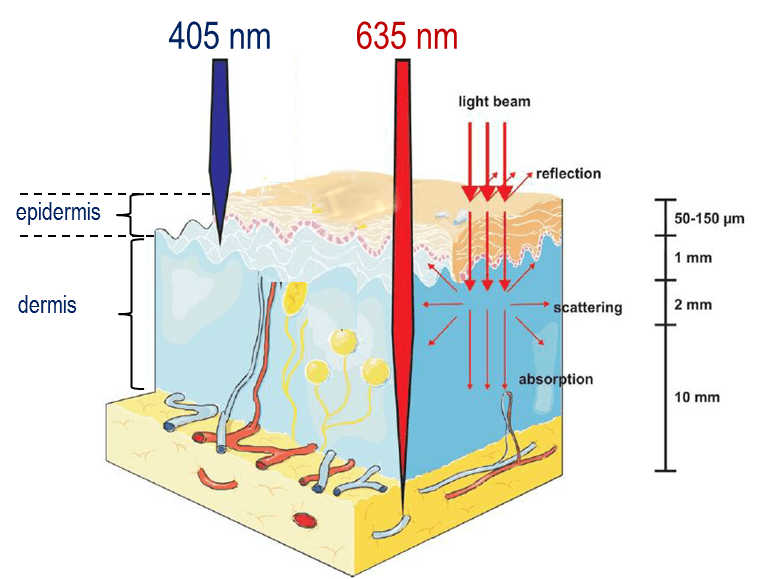
Photodynamic Therapy (PDT) PDT can be especially useful for lesions on the face and scalp, and when patients have multiple BCCs. Currently, this is used only for superficial SCC or Bowen’s disease. Topical 5-aminolevulinic acid (5-ALA) is applied to the lesions at the physician’s office. This solution is preferentially absorbed by the cancerous lesions, including those not visible with the naked eye. After one hour of incubation time, those medicated areas can be activated by light using intense pulsed light or blue or red light. This treatment selectively destroys SCCs while causing minimal damage to surrounding normal tissue. Some redness and swelling can result from this therapy. While insurance companies may pay for this method (using the destruction of malignant lesion code), they may not pay for the 5-ALA solution which has significant cost associated ($300-450 per application). Thus, this method may result in some out-of-pocket costs. This method has been shown to have excellent long-term cosmesis, and treatment of the full face may reduce the risk of development of new lesions in the future. Dr. Rosenberger does offer this innovative treatment method in her office.
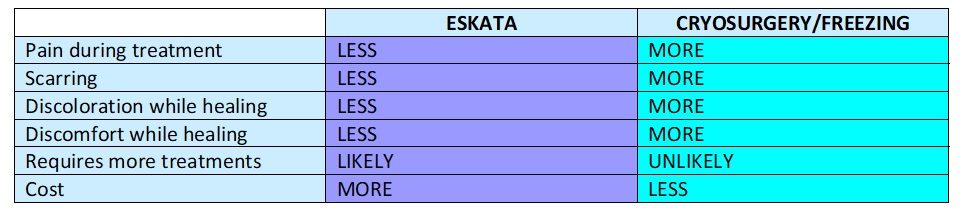
Cryosurgery Liquid nitrogen is applied to the growths with a spray device. This freezes them without requiring any cutting or anesthesia. They subsequently blister or become crusted and fall off. The procedure may be repeated to ensure total destruction of malignant cells. Some temporary redness and swelling can occur. In some patients, the pigment may be lost. This method is rarely used because it has a high recurrence rate.
Radiation X-ray beams are directed at the tumor. Total destruction usually requires several treatments a week for a few weeks. This is ideal for tumors that are hard to manage surgically and for elderly patients who are in poor health. This method is complicated by the side effects of radiation. This would require a referral to a radiation specialist.
Laser Surgery and Chemical Peels The skin’s outer layer and variable amounts of deeper skin are removed using a carbon dioxide or erbium YAG laser. Only deeper chemical peels (such as TCA) are able to treat superficial skin cancers. Lasers and chemical peels are effective for removing actinic cheilitis from the lips and precancers from the face and scalp. With a laser, the risks of scarring and pigment loss are greater than with other techniques. This method is also only effective for the most superficial tumors and is not a well-accepted method. Dr. Rosenberger does not perform laser or chemical peels for skin cancers.
Cemiplimab is a type of immunotherapy known as a checkpoint blockade therapy, which works by harnessing the power of the immune system to battle cancer. This is reserved for the most advanced and treatment-resistant cases.
After you have been diagnosed and treated for squamous cell carcinoma
What is my risk of the tumor recurring or spreading? The risk of non-melanoma skin cancer spreading or metastasizing to other parts of the body is low. However, the tumors can recur locally if not totally removed or a new lesion can occur adjacent to the previous one or in a new location.
What is my risk of developing another skin cancer in the future? One in five Americans develops skin cancer some time in their life. Once someone has one type of skin cancer, they have a further increased risk of developing both non-melanoma and melanoma skin cancer in the future.
What can I do to prevent new lesions now? It is important to continue aggressive sun protection and sun avoidance when possible. Dr. Rosenberger likes to see her skin cancer patients at three months, six months, and one-year intervals following diagnosis and treatment of skin cancer. At these visits, we will be looking for recurrence as well as monitoring for the development of new lesions.
Do my family members now have an increased risk of developing skin cancer? There are a few rare genetic syndromes where family members all develop high numbers of skin cancers. However, most non-melanoma skin cancers do not have increased for immediate family members by a direct specific gene. That being said, we inherit many characteristics from our parents, including skin color, eye color, and hair color which may increase one’s propensity to develop skin cancer. Plus, the family that plays in the sun together gets skin cancer together. For instance…Dr. Rosenberger’s father has had basal cell carcinoma. Dr. Rosenberger inherited her fair skin and tendency to freckle from her father. Dr. Rosenberger spent time at the beach with her family. Dr. Rosenberger developed her first basal cell carcinoma at age 30.
If you would like to learn about the other major types of skin cancer, check out our previous posts.
Portions of this handout are derived from a similar article by the Skin Cancer Foundation. To read even more about Squamous Cell Carcinoma, check out their site.
Skin Cancer Foundation – Squamous Cell Carcinoma 101
_________________________________
If you know someone who may find this article helpful, please share it with them! Follow us on social media this week, and subscribe to our growing YouTube channel! If you would like to receive these posts in your email inbox, Subscribe to our Site.











 Laser Vein Reduction Treatments
Laser Vein Reduction Treatments



 DP Dermaceutical Products
DP Dermaceutical Products





