Can you have BOTOX while taking oral antibiotics?
Can you have BOTOX while taking oral antibiotics?
Every so often a patient asks a question that gives me and my staff a pause. Hmmm? My immediate answer when a patient called to ask this question was OF COURSE. But then, the internet said otherwise, so what’s the real scientific answer?
Turns out the package insert that comes with BOTOX says this… LINK https://www.abbvie.ca/content/dam/abbvie-dotcom/ca/en/documents/products/BOTOXCOSMETIC_PI_EN.pdf
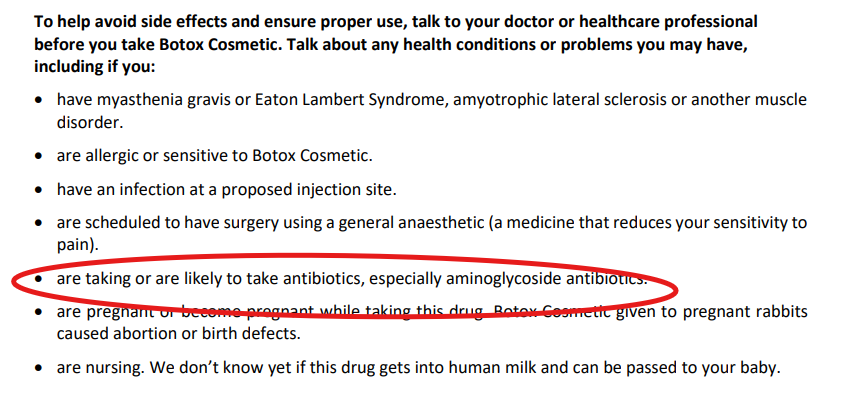
I did a lot of research for this post. The recommendation of avoiding aminoglycoside antibiotics is based on a 1981 report that these antibiotics worsened Botulinum symptoms. Theoretically, these antibiotics could make BOTOX more effective than desired. Aminoglycoside antibiotics are Amikacin, Gentamicin, Neomycin, Plazomicin, Tobramycin and Streptomycin. The reference for that article is here.
Santos JI, Swensen P, Glasgow LA. Potentiation of Clostridium botulinum toxin aminoglycoside antibiotics: clinical and laboratory observations. Pediatrics. 1981 Jul;68(1):50-4. PMID: 7243509.
There was one case I found of a patient that developed hives while on a B lactam antibiotic after treatment with Chinese Botulinum Toxin
Feng W, Liu H. Urticaria-Like Hypersensitivity Reaction Following Botulinum Toxin Injection: A Case Report of Possible Interaction with β-Lactam Antibiotics. Int Med Case Rep J. 2025 Mar 20;18:367-371. doi: 10.2147/IMCRJ.S510203. PMID: 40129562; PMCID: PMC11932131.
Most other reports are AI generated from various non-scientific literature reports. I did find one other article that listed other drugs that could have a theoretical scientific interaction with Botulinum Toxins.
These included potentiation (more effective/ more weakness) with Aminoglycoside antibiotics, succinylcholine, curare, magnesium sulfate, quinine, calcium channel blockers, cyclosporine, muscle relaxants and penicillamine. Of these, calcium channel blockers are commonly used by patients. Calcium channel blockers include amlodipine, diltiazem, felodipine, isradipine, nicardipine, nifedipine, nisoldipine and verapamil.
Antimalarial medications such as hydroxychloroquine (Plaquenil) are a more common medications used by patients in the US. One study suggested that antimalarials may antagonize Botulinum toxin.
Simpson LL. The interaction between aminoquinolines and presynaptically acting neurotoxins. J Pharmacol Exp Ther. 1982 Jul;222(1):43-8. PMID: 6283072.
So what does all of this mean?
If you have been treated with Botulinum toxin while on one of these medications in the past and have not had any side effects, you’re good. Most botulinum toxin cosmetic effects wear off in 3-4 months.
If you are taking Plaquenil or a calcium channel blocker, we may want to do a test dose in your arm or dose your botulinum toxin very low to start.
If you are taking an Aminoglycoside antibiotic it is most prudent to avoid botulinum toxin treatments until those medications have cleared your system which should be within a few days of stopping the antibiotic.
This is why medicine is still interesting after over 20 years. Patients ask good questions, and I get to find the answers.
As a general aside, I have been receiving and administering Botulinum toxin to patients for over 20 years. To my knowledge, I have not seen a medication related side effect. However, it is well known that everyone responds to botulinum toxin differently. This is why I always start “gentle” and lean to the side of “underdoing not overdoing”. There are probably lots of things that affect how a patient responds to botulinum toxin, so going slow is always the prudent path.
If you know someone who may find this article helpful, please share it with them! Follow us on social media this week, and subscribe to our growing YouTube channel! If you would like to receive these posts in your email inbox, Subscribe to our Site.
