

An actinic keratosis (AK) is a scaly or crusty bump that arises in sun exposed areas. Usually these are pink and white scaly, but occasionally can be brown. They often will vary in thickness over time as dead skin builds up and flakes off. Early on, it may disappear only to reappear later. If a lesion comes and stays for three months, or gets tender to touch, it is time to take action.
AKs are what we call precancer spots, meaning that the skin cells are growing abnormally on the surface of the skin. If the AK is allowed to progress, the abnormal cells will grow deeper in the skin and advance to a Squamous Cell Carcinoma. If you have AKs, it indicates that you have sustained sun damage and could develop any type of skin cancer – not just squamous cell carcinoma. The more AKs you have, the greater the chance that one or more may turn into skin cancer.
People who have fair skin, blonde or red hair, and/or blue, green, or gray eyes are at greatest risk. But even darker-skinned people can develop AKs if exposed extensively to the sun without protection. Patients develop more AKs as they age. Individuals whose immune systems are weakened are also at higher risk.
Actinic Keratoses (AKs) – Treatment Options
There are many effective methods for eliminating AKs. Because these lesions are so common and often numerous, it is often not necessary to biopsy each of these lesions. Lesions are often treated without prior biopsy. Most of the treatment methods below have similar efficacy. Therefore, treatment method is decided mainly by patient preference and insurance coverage issues. Pain or discomfort is usually minimal with most techniques, and there is rarely much pain afterwards. Almost all patients will require continual or intermittent treatment because new lesions continue to develop over time due to sun damage from the past.
THERAPY OF INDIVIDUAL LESIONS
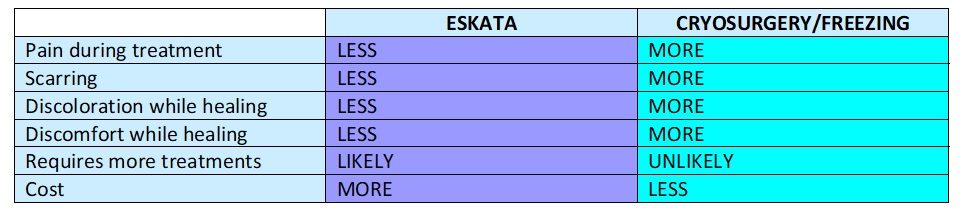
Cryosurgery Liquid nitrogen is applied to the growths with a spray device. This freezes them without requiring any cutting or anesthesia. They subsequently blister or become crusted and fall off one to four weeks after treatment. The procedure may need to be repeated to ensure total destruction of malignant cells. One day after treatment, lesions will have a blistery scab. This is the most used method for treating AKs. This method is preferred for those with only a few lesions, thicker spots and lesions in areas not accessible or easily treatable with topical creams. The advantage is that this procedure is completed in minimal time in the office. There is some minimal pain during the freezing process. The biggest disadvantage is that this method can leave a pale mark behind.
FIELD THERAPY
Field therapy is where we treat a whole area where multiple AKs are located. By treating the whole area, we can treat both lesions we see and ones that are lying in wait for the future. This is the best way to “wipe your slate clean”. Field therapy options vary in efficacy somewhat, but most clinical trials show that any of the treatments listed below will remove approximately 75% of the lesions in a given area after a treatment course.
Topical Medications A number topical medications are approved for the treatment of actinic keratoses . Topical medications can have excellent cosmetic outcomes, but require patient compliance with both application of the medicine and the medication side effects. This method is best used on large superficial lesions, multiple lesions (>25) and lesions where cosmesis is a primary issue.
5-Fluorouracil (5-FU, Efudex, Tolak or Carac) is a chemotherapeutic topical cream that can be applied to the area once or twice a day for up to four weeks. 5FU inhibits a cell’s ability to reproduce. AK cells grow faster than normal skin cells, which means they absorb the medication faster than the surrounding healthy cells. During application it causes inflammation with red crusted sores and then sloughing, or shedding, of these abnormal cells. This irritation is common and expected and is a sign that the treatment is working. It is important that you not stop therapy. The more AKs and abnormal cells that you have, the more redness and inflammation you can expect during treatment. After treatment, the irritation should subside in approximately 2 weeks. During this treatment, people with many lesions may not feel comfortable going out in public. Carac is applied once a day, while Efudex or generic 5FU is applied twice a day. These creams are applied for 4 weeks, so skin is usually red, scabby and crusty for 6 weeks total.
Imiquimod (Aldara, Zyclara) was originally designed to treat warts, but studies quickly showed that this medication could induce our own immune system to fight off skin cancer cells. Side effects and treatment course and the unsightly appearance during treatment is similar to 5FU. This medication is also FDA approved to treat superficial basal cell carcinomas.
Solaraze combines hyaluronic acid and an anti-inflammatory medication diclofenac. This medication is used twice a day for 3 month intervals. There is less irritation than seen with 5FU and only rarely do open sores develop. However, this is overall less effective than 5FU or Imiquimod in lesion clearance.
Tretinoin (RetinA) and other topical retinoids have been used for many years for acne, rosacea, anti-aging and more. Patients using these medications on a continual basis have seen both clearance of thinner AKs as well as fewer lesions developing with time. Although tretinoin is much less aggressive overall, it is safe to use nightly long term. Users experience redness and peeling of the skin during the first 6 to 12 weeks of use. AKs turn red and peel off in the first few months of use. Lesions are usually not open sores or as painful as with 5FU or Imiquimod. However, many insurance companies will not cover this medication because it is so commonly used for cosmetic anti-aging properties.
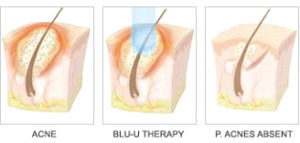
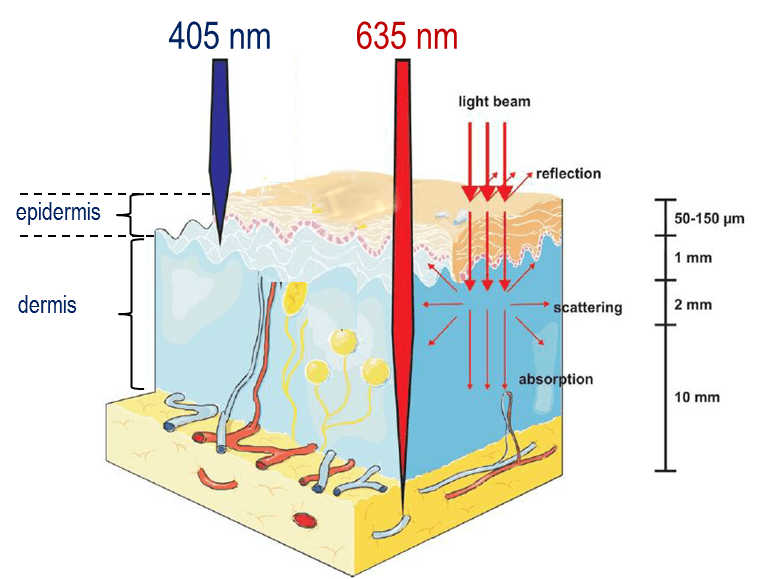
Photodynamic Therapy (PDT) PDT can be especially useful for lesions on the face and scalp, and when patients have multiple AKs. Topical 5-aminolevulinic acid (5-ALA) is applied to the lesions at the physician’s office. This solution is preferentially absorbed by the cancerous lesions, including those not visible with the naked eye. After approximately one hour incubation time, the patient sits under a LED light. Then there is an interaction between the light and the 5-ALA that is in the abnormal cells that causes death for the abnormal cells. This treatment selectively destroys AKs while causing minimal damage to surrounding normal tissue. Patients have what appears to be a decent sunburn that peels for 7 days. Overall, there is less down time than with the creams. This treatment also helps acne, rosacea and has superb cosmetic benefits. While most insurance companies including medicare pay for this method, they may not pay for the 5-ALA solution which has significant cost associated ($450 per applicaton). Medicare DOES cover the solution. We have some options for reducing cost of the solution which we can discuss with you.
After you have been diagnosed and treated for Actinic Keratoses
Does every AK need to be treated immediately? Studies show that only a small percentage of AKs will develop into skin cancers. Many lesions will be repaired during the skin’s normal repair process as we shed and renew our skin each month. However, all persistent and thick lesions should be treated. Treating AKs as they occur on a regular basis or using one of the topical creams above can greatly reduce the risk of the lesions becoming skin cancers in the future.
What is my risk of developing a skin cancer in the future? One in five Americans develop a skin cancer some time in their life. Once someone has AKs they have an increased risk of developing both non-melanoma and melanoma skin cancer in the future.
What can I do to prevent new lesions now? It is important to continue aggressive sun protection and sun avoidance when possible. Dr Rosenberger likes to see her skin cancer and actinic keratosis patients at six months and one-year intervals following diagnosis and treatment. At these visits we will be looking for recurrence as well as monitoring for the development of new lesions. For prevention, and to reduce the number of lesions, both the topical creams and photodynamic therapy are suggested to be chemopreventitive. One recent study demonstrated that using a sunscreen with DNA repair enzymes daily decreased the development of actinic keratosis when used on a regular basis.
Do my family members now have increased risk of developing a skin cancer? There are a few rare genetic syndromes where family members all develop high numbers of skin cancers. However, most non-melanoma skin cancers and actinic keratoses do not have increased for immediate family members by a direct specific gene. That being said we inherit many characteristics from our parents, including skin color, eye color and hair color which may increase one’s propensity to develop a skin cancer. Plus, the family that plays in the sun together gets skin cancer together. For instance…Dr Rosenberger’s father has had basal cell carcinoma. Dr Rosenberger inherited her fair skin and tendency to freckle from her father. Dr Rosenberger spent time outside with her family. Dr Rosenberger developed her first basal cell carcinoma at age 30.
___________________________________________________
If you know someone who may find this article helpful, please share it with them! Follow us on social media this week, and subscribe to our growing YouTube channel! If you would like to receive these posts in your email inbox, Subscribe to our Site.











 Laser Vein Reduction Treatments
Laser Vein Reduction Treatments



 DP Dermaceutical Products
DP Dermaceutical Products





